COVID-19 is primarily a respiratory infection; however, there are multiple examples of multi-organ and systemic dysfunction associated with this infection.1 In addition to lung damage, it appears that the virus affects the lining of blood vessels, potentially leading to clotting, embolization, and organ damage. In a recent study by Hirsch et al,2 acute kidney injury (AKI) was reported to occur at a high rate in hospitalized COVID-19 patients. Our examination of EHR data confirmed these findings and also revealed an increased incidence of AKI in COVID-19 patients with hypertension, diabetes, or COPD, as well as in patients on mechanical ventilation.
In this study, we looked at the incidence of AKI in 36,396 adult patients who were admitted for COVID-19 and had either been discharged or died, as of June 24, 2020. We counted only the first admission for patients with multiple COVID-19 admissions. Additionally, patients with chronic kidney disease or end stage renal disease were excluded from analysis, as baseline serum creatinine (an important measure in our definition of AKI) is usually elevated in these patients. These criteria for our patient population slightly differed from those employed by Hirsch et al, notably in their inclusion of patients that were still hospitalized at the time of the study and patients with chronic kidney disease. In our sampled population, we found that the incidence of AKI was 31.3%, similar to the high rate of AKI (36.6%) reported by Hirsch et al.2
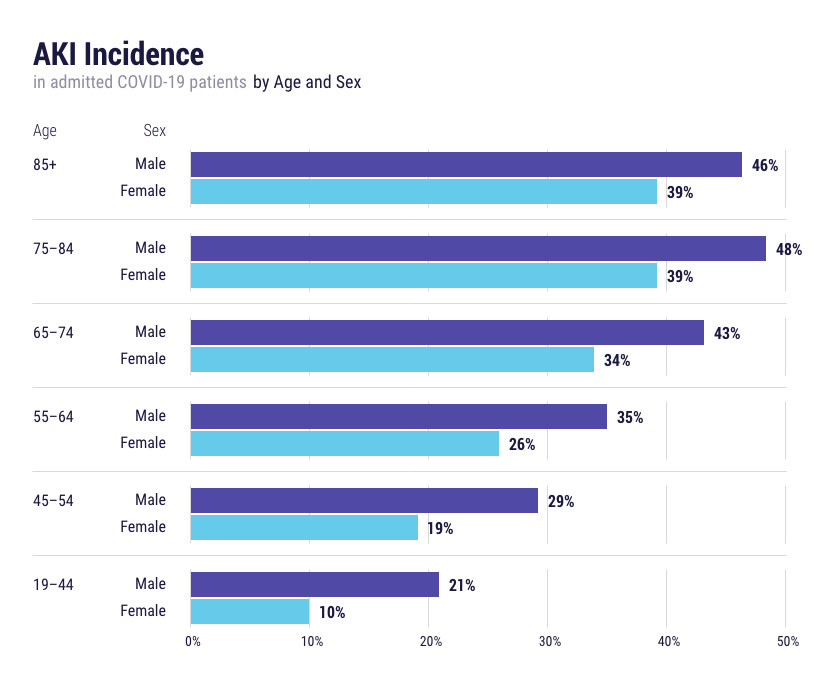
We also wanted to see if there was a relationship between age or sex and the incidence of AKI in COVID-19 admitted patients. As shown in Figure 1, we saw that the rate of AKI increased with age and was also higher in males.
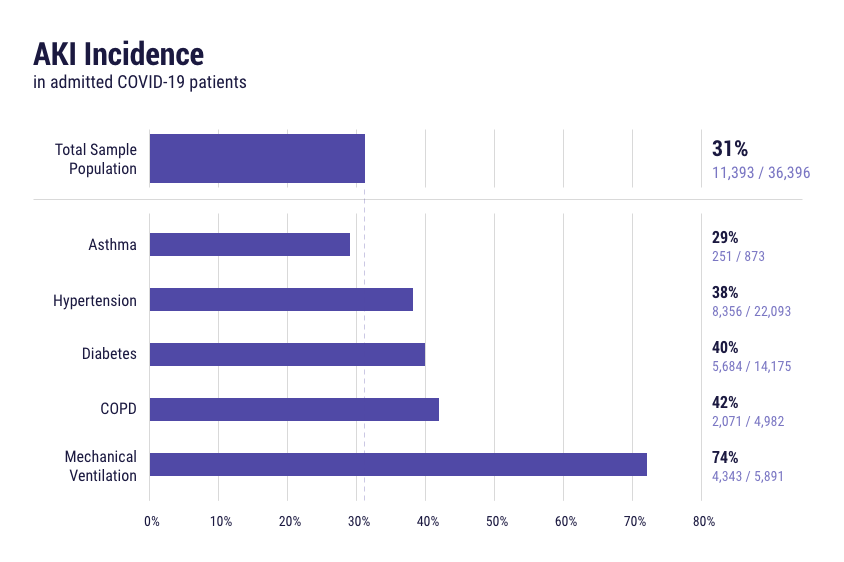
Next, we looked at how the incidence of AKI changed in subsets of patients with particular comorbidities or disease outcomes. As shown in Figure 2, we found the rate of AKI to be higher in patients with hypertension, diabetes, or COPD. Notably, the incidence of AKI in patients who were mechanically ventilated was 74%. While not as high as that reported by Hirsch et al2 (89.7%), this nonetheless indicates a strong relationship between respiratory failure and AKI.
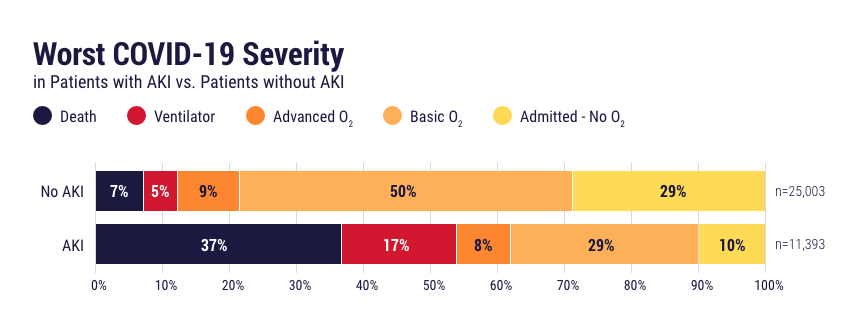
Finally, we investigated the worst COVID-19 severities for those patients who developed AKI during their admission. As shown in Figure 3, the development of AKI was associated with a higher severity of illness and poorer outcomes (e.g., death in 37% of patients), when compared to hospitalized patients who did not develop AKI.
Overall, the findings in this study are very similar in magnitude to the findings reported by Hirsch et al.2 These results further support the high incidence of AKI in COVID-19 patients and also highlight the association between respiratory failure and the development of AKI.
Data are pooled from 43 health systems representing 396 hospitals that span 20 states and cover 30 million active patients.




