By early December 2020, over 100,000 patients are hospitalized with COVID-19 in the United States. Two key variables in understanding the stress to the health system due to new COVID-19 hospitalizations are the availability of staff and ICU beds. We analyzed these for 809 hospitals in metro, suburban, and rural settings from July 2020 to December 3, 2020.
Nurse Staffing Impact
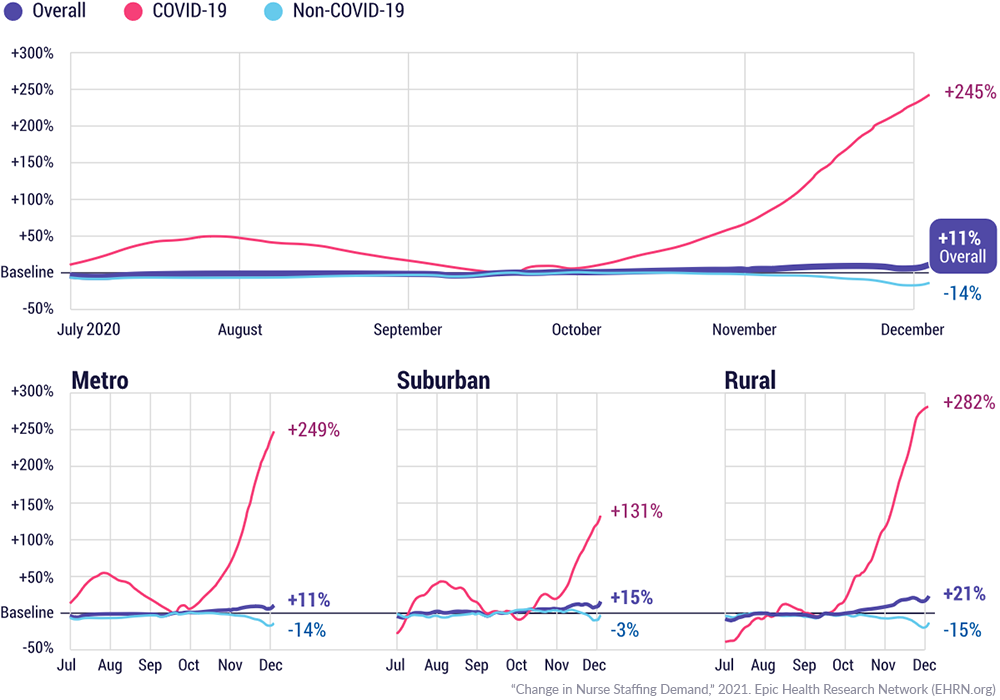
Nationwide, we estimate that 77,500 nurses are directly caring for COVID-19 patients each day, compared with only 22,500 nurses in mid-September, an increase of 245%. Metro and rural hospitals increased at a rate nearly double that of suburban hospitals (249%, 282%, and 131% respectively). Non-COVID staffing needs are down, but taken together, COVID-19 and non-COVID-19 nurse staff demands have increased by an additional 26,000 nurses (11%) per day doing direct patient care that can be attributed to increased COVID-19 hospitalizations. Changes were normalized against a mid-September 2020 baseline due to low COVID-19 hospitalizations and near pre-pandemic levels of occupancy in that time period.
ICU Beds Impact
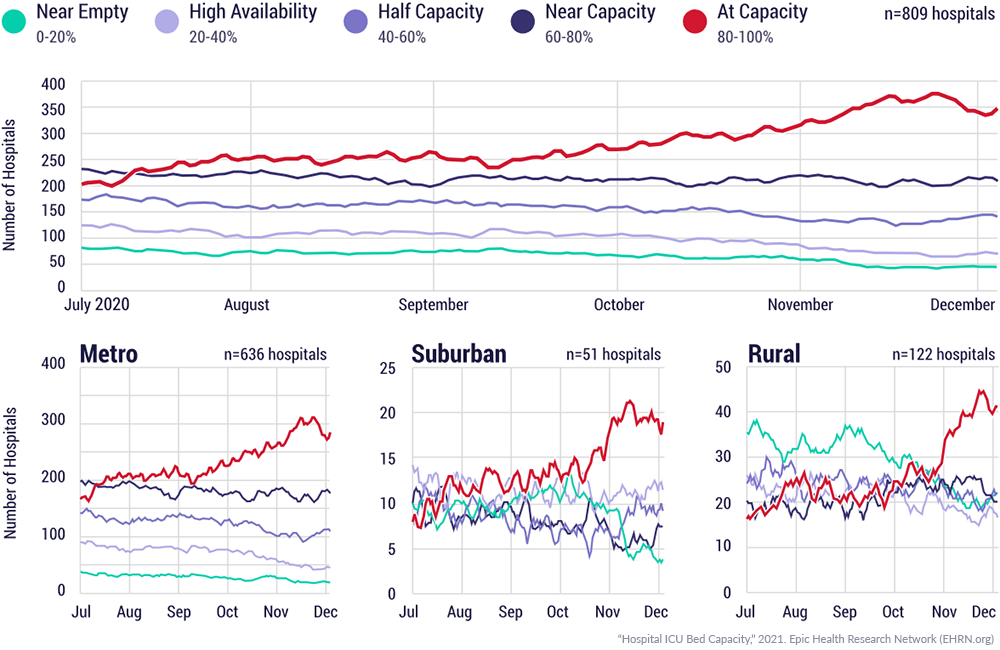
Health systems have created additional physical bed capacity to handle less severe COVID-19 cases. However, critically ill patients still need fully-equipped intensive care units (ICU). We trended the number of ICUs by occupancy and found that there was a 90% increase in the number of hospitals at capacity (80-100% occupancy) in their ICUs.
Rural hospitals with smaller ICUs are reaching capacity more quickly than metro and suburban hospitals. From July to early October, our largest grouping of rural ICUs showed plenty of availability (0%-20% occupancy), now our largest grouping of rural ICUs are at capacity (80-100% occupancy). Rural ICU staffing also increased the most, increasing 46% since mid-September, compared to only a 24% increase for metro and suburban ICUs.
Analysis and Methods
Analysis was completed using Pulse Central, a portal created by Epic to aggregate real-time COVID-19 metrics for public health reporting including infections, bed availability, and hospitalizations. All data is aggregated daily down to the zip code of the location of the care facility. We mapped the zip codes to core-based statistical area (CBSA) type and grouped “Metro – Central” as metro, “Metro – Outlying” as suburban, and “micro” or null as rural. The data set included 183 unique healthcare organizations representing 809 hospitals reporting from July 2020 to December 2020.
To calculate the direct nursing care needs, we first determined a baseline hospital occupancy level to measure the overtime occupancy change against, which we chose to be the week of September 11th. We chose that week because it had the lowest number of COVID-19 patients in beds during our reporting period and hospitals occupancy was close to September 2019 benchmarks from our dataset.
Next, to determine the increased nursing needs, we used industry standard staffing ratios to apply to the increase in patient hospitalizations. We used a 4 patients to 1 nurse ratio for non-ICU acute patients (both with and without a COVID-19 infection), 2 patients to 1 nurse ratio for non-COVID-19 ICU patients, and 1.25 patients to 1 nurse ratio for COVID-19 ICU patients. Then to understand the daily staff need, we doubled the staff needs assuming that we needed a minimum of 2 nurse staff to work a 24-hour day (assuming 12-hour shifts). This estimate is conservative, as not all nurses will be working 12-hour shifts.
After normalizing the increase in hospitalizations to an increase in nursing staff, we took the 29,174 COVID-19 hospitalizations in our data set on December 3, 2020 and extrapolated the staffing needs to the 100,000 COVID-19 hospitalizations reported nationally the same day, which involved multiplying staffing by 3.4 to arrive at a national estimate of nurse staff needed for COVID-19 (77.5k nurses).
Finally, to arrive at the total change nationally in staffing (26k nurses) we attribute to COVID-19, we measured the increase in COVID-19 staffing (55k nurses) as of December 3, 2020 compared to the September 2020 baseline (22.5k nurses), then we further subtracted the estimated staff needs from the drop in non-COVID-19 hospitalizations (29k nurses).
When estimating staffing, we only looked at the direct nursing care assignments. Many staff are involved in the care delivery system that do not go into this number. We are unable to measure additional variables that can add strain to the health system, such as staff being unavailable due to COVID-19 infections or stress associated with caring for a COVID-19 patient.




