Public policy decisions in the United States have relied on epidemiologic models that predict the course of the COVID-19 pandemic. These models rely on certain assumptions about the impact of the disease on the population, such as inpatient length of stay and ICU days. The model published by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington in Seattle has received the most media attention. Some of its assumptions are based on data from Wuhan, China from December 2019.1
We compared the IHME assumptions to the median inpatient length of stay and ICU days in a sample of 94,875 admissions across 21 U.S. states.
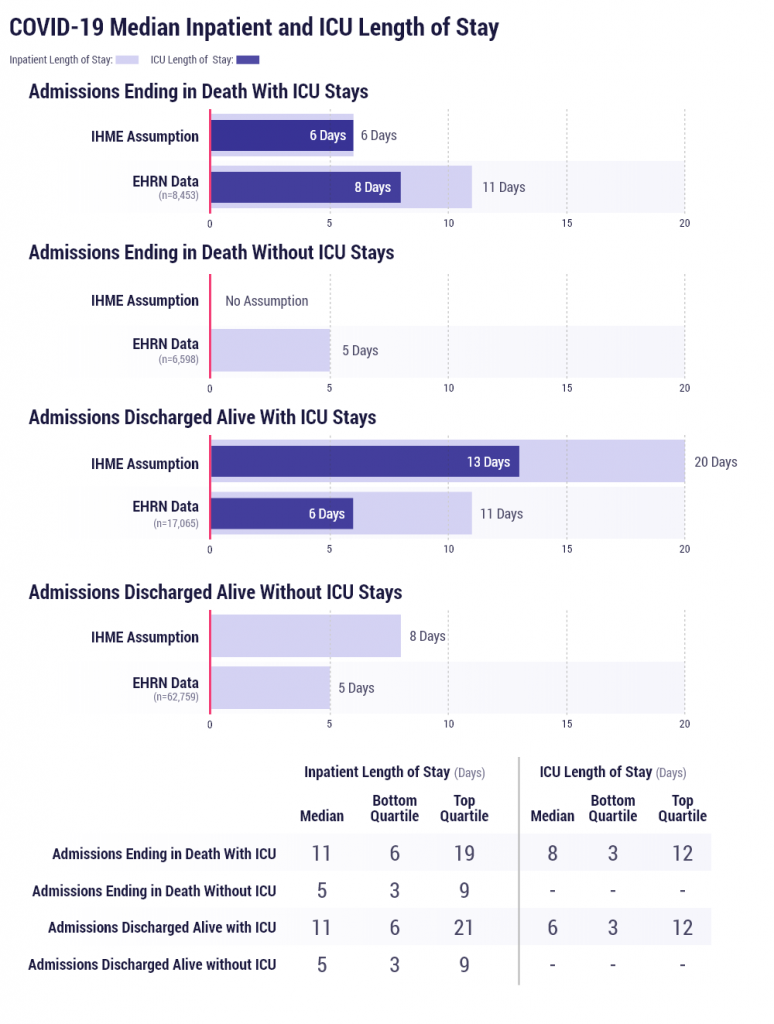
Medians were calculated separately for patients who were discharged from the hospital and those who died in the hospital, and those who spent any time in critical care and those who did not. All lengths of stay were expressed in whole numbers. We present the data along with the 1st and 3rd quartiles for each group in Figure 1, which indicates the distribution of length of stay in the sample.
Figure 2 includes data from the same set of 94,875 admissions further stratified by age.

These median estimates differ from IHME assumptions. If these differences indeed represent real clinical differences, then they may be due to a change in the characteristics of the COVID-19 disease, or improvement in management, as patients who died are surviving longer and patients who survived are spending shorter periods in both levels of hospital care.
Data are pooled from 54 healthcare organizations representing 526 hospitals that span 21 states and include 94,875 COVID-19 related admissions as of July 29, 2020.




